Research Article
Knowledge Regarding Selected Infectious Diseases, Their Prevention and Management among Adults in Selected Rural Community, Gurugram, Haryana
922
Views & Citations10
Likes & Shares
Background: Despite enormous advances in medical sciences and their applications in public health, infectious diseases remain a central challenge for public health in the twenty-first century.
Aim of the work: The present study aimed to assess the knowledge regarding selected infectious diseases, their prevention & management among adults in selected rural community, Gurugram, Haryana, India.
Methodology: A descriptive research approach was adopted with convenient sampling method. A total of 100 samples were selected for the present study and data was collected through a structured questionnaire. Objectives of the study were to assess the knowledge regarding prevention and management about selected infectious diseases and to find out association between knowledge score regarding prevention and management of infectious diseases and selected socio- demographic variables.
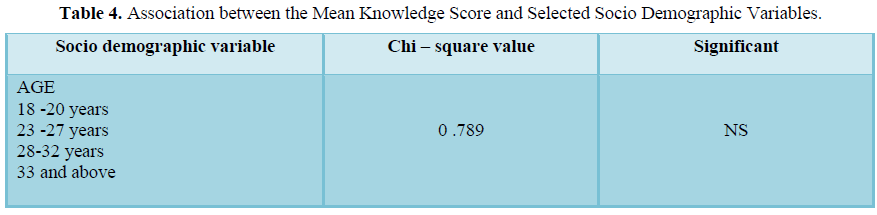
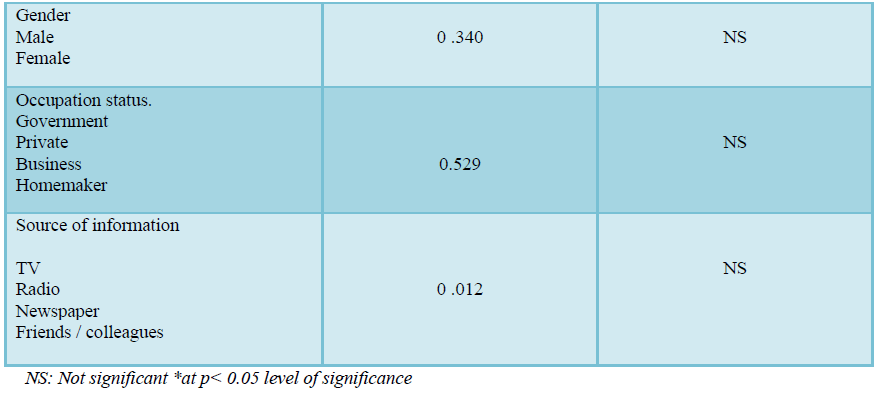
Results: Findings of the present study showed that 76% adults were having good knowledge while 65.4% were having moderate knowledge regarding selected infectious disease their prevention and management. Chi square test revealed that none of the socio-demographic variable was associated with the level of knowledge regarding selected infectious diseases.
Conclusion: The study findings showed that there was lack of knowledge and awareness regarding selected infectious diseases among the adults. So, this study recommends creating health education materials and mass awareness programmes for the up gradation of knowledge regarding infectious diseases among adults.
Keywords: Knowledge, Infectious diseases, Prevention and management, Adults
INTRODUCTION
The lack of treatment of infectious diseases in developing countries is a tragic problem and one of the most serious challenges that the world must face at the beginning of this century. Hundreds of millions of people suffer from transmissible diseases for which treatments exist but for which the patients are not receiving treatment [1]. Infectious diseases are leading causes of death in developing countries. According to data from the World Health Organization, 1.2% of total deaths from infectious and parasitic diseases occurred in industrialized countries, compared to 43% in developing countries. Women in developing countries disproportionately suffer from a host of infectious diseases, including tuberculosis, upper respiratory tract infections, skin infections, visceral leishmaniasis, malaria, sexually transmitted infections and HIV/AIDS. Poverty, poor education, low health knowledge, poor infrastructure, geographic factors, life style and environmental factors (i.e., limited access to resources such as clean water) have been identified as primary factors contributing to the high incidence of infectious diseases among women in developing countries. Also, such women tend to have limited or no access to health care, be vitamin deficient, and have lower status in their communities. Often, infectious diseases may run a substantially longer course for women in developing countries because of stigma, family needs, and shame. Another important barrier to combating infectious diseases among women in developing countries is the lack of use and the misuse of prescription medication. A substantial percentage of women rely on traditional treatment methods.
When women do seek healthcare services and are prescribed medication, women frequently do not adhere to the dosage and quantities prescribed [2].
It is estimated that around nine percent of the population in the United States has been diagnosed with an infectious disease. Infectious diseases are caused by bacteria, viruses and other organisms and can be spread from person to person, through insect or animal bites, or through contaminated food or water. Some of the most common infectious diseases include HIV/AIDS, influenza, malaria, tuberculosis and hepatitis [3]. Each disease has its own characteristic organism and natural history from onset to resolution. Many infectious diseases may remain at a presymptomatic or subclinical stage without progressing to clinical symptoms and signs, but may be transmissible to other people. Even a subclinical disease may cause an immunological effect, producing immunity [4]. The potential for infectious disease to disturb or destroy human life still exists today, especially in low-income countries, but can also pose serious challenges in the high-income countries. This threat may increase as infectious diseases evolve and escape current human-developed control mechanisms. An agent of an infectious disease is necessary but not always sufficient to cause a disease or disorder. The infective dose is the quantity of the organism needed to cause clinical disease. A disease may have a single agent as a cause, or it may occur as a result of the agent in company with contributory factors, such as in socially deprived and undernourished populations or among immune compromised people who are vulnerable to the spread and development of the disease. A disease may be present in an infected person in a dormant form, such as TB, or a preclinical stage, such as poliomyelitis (polio) or HIV, without clinical paralytic disease in the case of polio or before clinical AIDS appears in the case of HIV. The virulence or pathogenicity of an infective agent is the capacity of an infectious agent to enter the host, replicate, damage tissue, and cause disease. Virulence describes the severity of clinical disease and may vary among serotypes or strains of the same agent [4]. Improvements in state and local public health infrastructure along with innovative and targeted prevention efforts yielded significant progress in controlling infectious diseases. Examples include a 30% reduction from 2001 to 2010 in reported U.S. tuberculosis cases and a 58% decline from 2001 to 2009 in central line--associated blood stream infections. Major advances in laboratory techniques and technology and investments in disease surveillance have improved the capacity to identify contaminated foods rapidly and accurately and prevent further spread. Multiple efforts to extend HIV testing, including recommendations for expanded screening of persons aged 13-64 years, increased the number of persons diagnosed with HIV/AIDS and reduced the proportion with late diagnoses, enabling earlier access to life-saving treatment and care and giving infectious persons the information necessary to protect their partners [5].
As of 2010, around 46 percent of deaths by communicable diseases in India were due to diarrheal diseases, while 29 percent were due to respiratory infections. This was a high share of deaths due to communicable diseases in the country with respect to its population [6].
Research Statement
A study to assess the knowledge regarding selected infectious diseases, their prevention and management among adults in selected rural community, Gurugram, Haryana, India.
Objectives of the study
- To assess the knowledge regarding prevention and management of selected infectious diseases.
- To find association between knowledge score regarding prevention and management of infectious diseases and selected socio- demographic variables.
Hypothesis
H1: - There will be significant difference in knowledge regarding selected infectious disease their prevention and management among adults.
H2: - There will be significant associations between knowledge level regarding selected infectious diseases their prevention and management among adults and socio-demographic variables.
MATERIALS & METHODS
Research approach
Quantitative research approach was used in the present study.
Research design
Descriptive research design was used for the present study.
Research setting
Rural community of Budhera, Gurugram, Haryana.
Sampling technique
Convenient sampling technique was adopted for the present study.
Sample size
A total of 100 samples were selected for the present study.
Population
In present study, the population consists of adults in Rural Community, Budhera, Gurugram, Haryana.
Sample
The sample for present study comprised of adults of Rural Community, Gurugram.
RESEARCH DESIGN
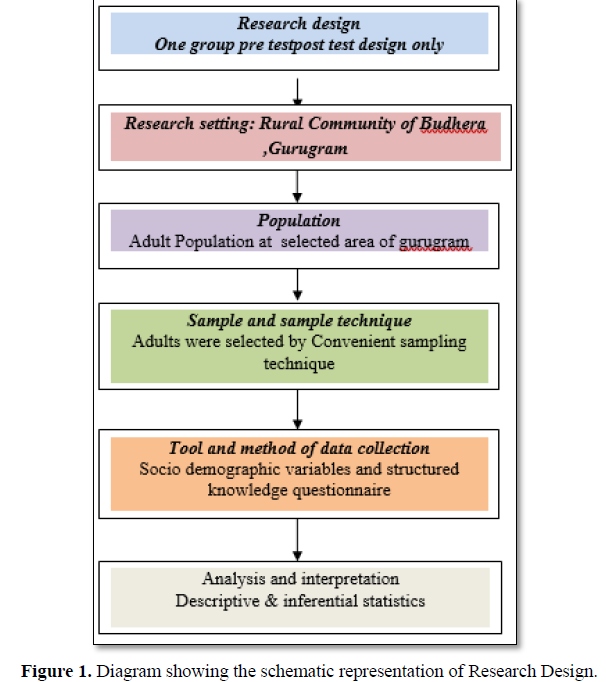
Schematic representation of research design (Figure 1)
CRITERIA OF SELECTION
Inclusion criteria
The participants full filing the inclusion criteria were included in study.
- Adults of age 18Years and above.
- 2. Willing to participant in study.
Exclusion criteria
Participants were excluded from study
- Not willing to participant in study.
- Not fulfilling the inclusion criteria.
Data collection tool and techniques
Tools were developing after doing extensive reviews of literature from book journals and taking opinion and suggestion from guide and experts.
The tools consist of 2 selection:
TOOL 1: Personal profile
TOOL 2: Structure knowledge questionnaires to assess the knowledge regarding selected infectious disease their prevention and management among adults structured questionnaire was formulated. The knowledge questionnaire consists of 30 MCQ question with one correct answer.
RESULTS
Section A
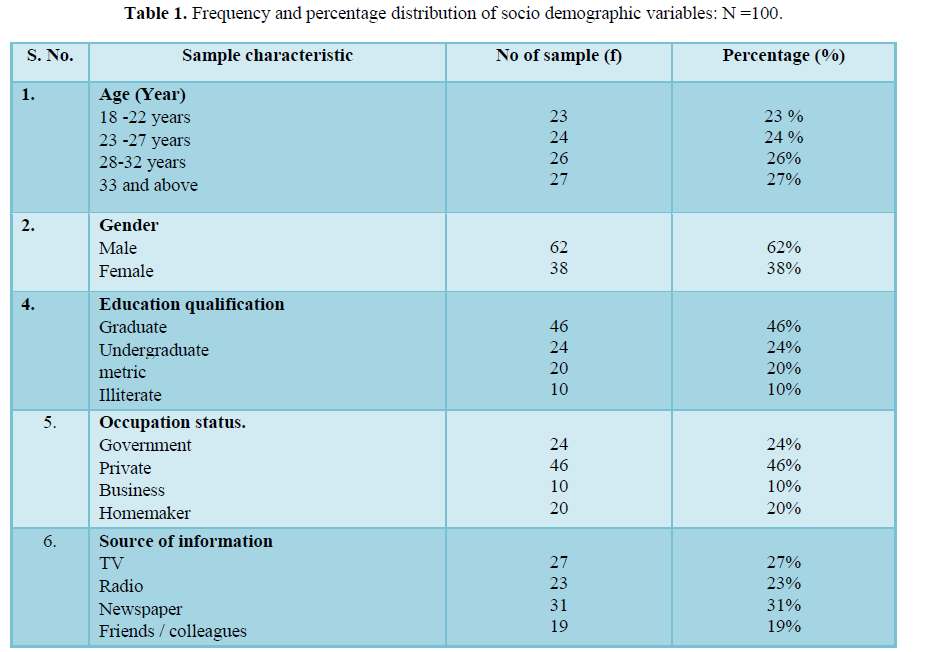
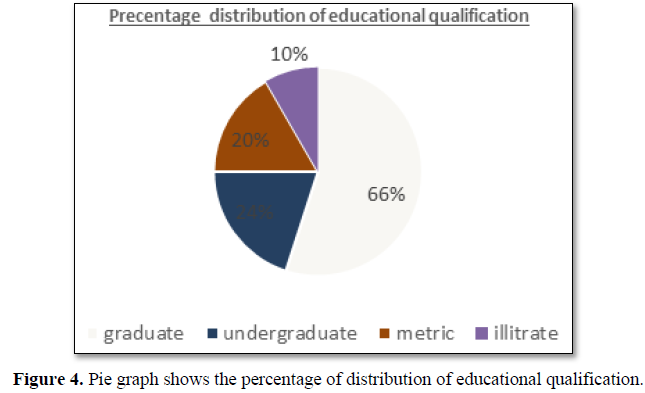
Data presented in Table 1 depicts that almost half 23% of the participants of the total samples were in the age group between 18-22 years of age, 24% of the participants were in the age group between 23-27 years of age. 26% of the participants were in the age group between 28-32 years of age and 27% of participants were in the age group between 33 and above 62% of the participants were male and 38% participants were female. Out of 10% of the participants were illiterate, 46% of the participants were having graduate education, 24% of the participants were having high undergraduate and 20% of the participants were metric. Out of total10% of the participants were having self-business, 20% of the participants were homemaker, 46% of the participants were private employee and 24% of the participants were government employee.
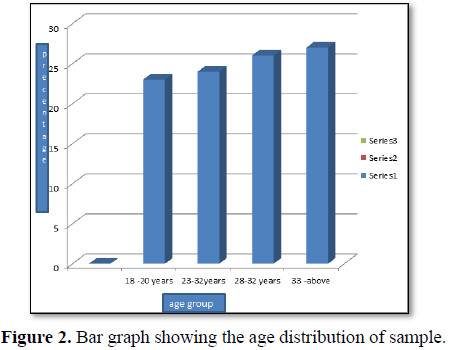
Age Distribution
Figure 2 shows that 23% of the participants of the total samples were in the age group between 18-22 years of age, 24% of the participants were in the age group between 23-27 years of age. 26% of the participants were in the age group between 28-32 years of age and 27% of participants were in the age group between 33 and above.
The data presented in Figure 3 shows that majority 62% of the study participants were male and 38% participants were female.
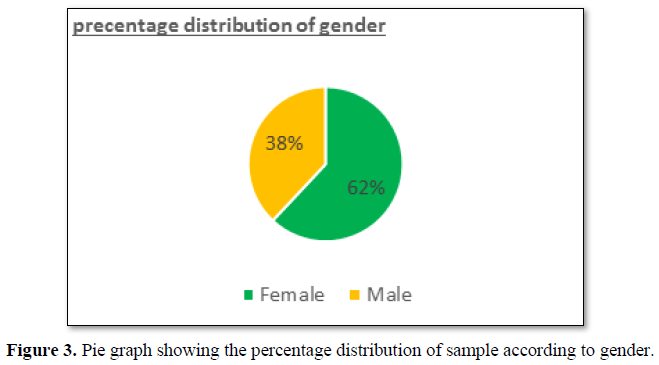
Figure 4 depicted that 10% of the participants were illiterate, 46% of the participants were having graduate education, 24% of the participants were having high undergraduate and 20% of the participants were metric.
Distribution of the participants according to their occupation status
In Figure 5, 10% of the participants were having self-business, 20% of the participants were homemaker, 46% of the participants were private employee and 24% of the participants were government employee.
Figure 6 depicted that source of information through TV was 27%, via radio 23%, newspaper 31% and friends /others 19%.
Section B
Table 2. Shows that distribution of level of knowledge Poor knowledge having Frequency 31 percentage 31%, Average knowledge having 51 and Frequency percentage 51%, good knowledge having Frequency 18 and Frequency percentage 18%.
Table 3 shows the distribution of level of age of Poor knowledge (20-25 years) 18, (26-30 years) 8, (31-35 years) 6 and Average knowledge (20-25 years) 16, (26-30 years) 14, (31-35 years) 12 and Good knowledge (20-25 years) 11, (26-30 years) 11, (31-35 years) 4.
Figure 7 shows the frequency distribution of gender with level of knowledge shows that poor knowledge shows that male 18 and female 16, Average knowledge male 16 and female 17, Good knowledge male 21 and female 12
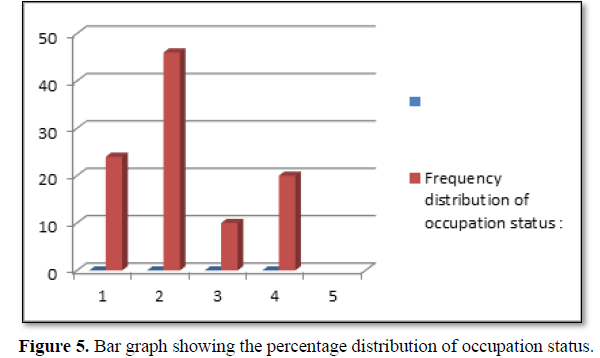
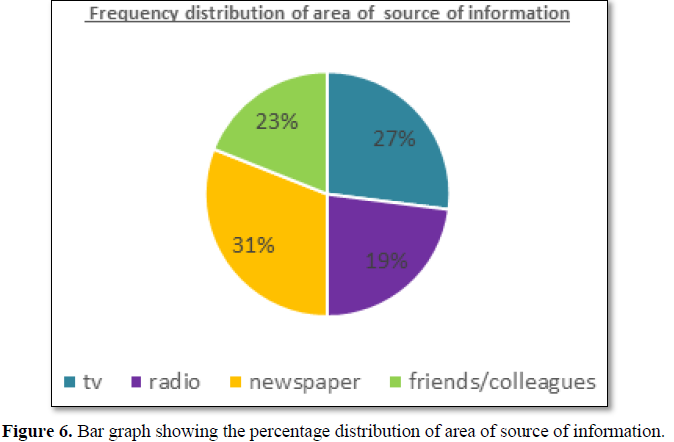
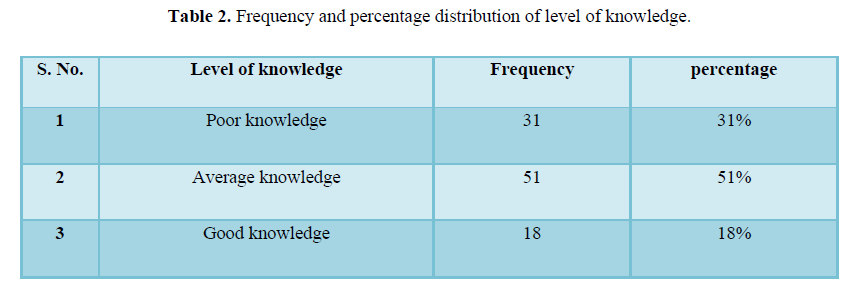
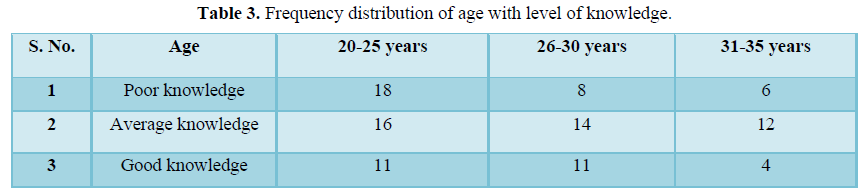
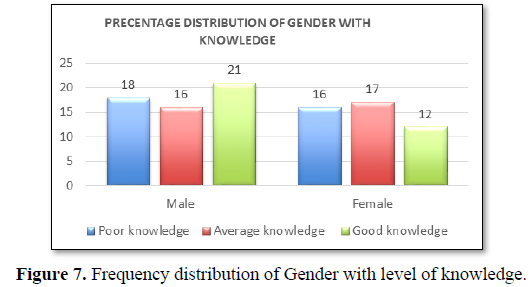
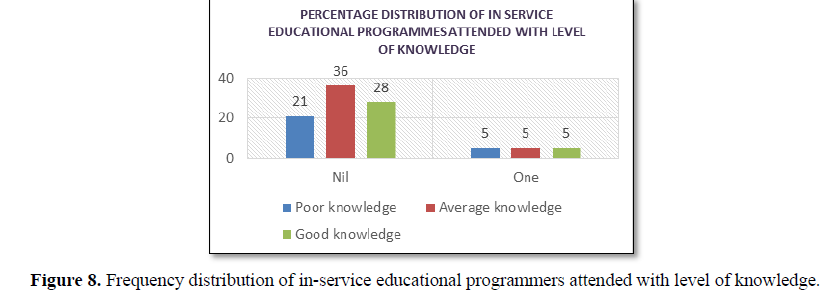
Figure 8 shows the frequency distribution of in-service educational programmers attended with level of knowledge shows that Poor knowledge nil 21 and one 5, Average knowledge nil 36 and one 5, Good knowledge nil 28 and one 5.
NURSING IMPLICATIONS
Nursing education
The study has an important implication in nursing education and other fields. One of the leading functions of nursing is to impart education with newer knowledge on infectious diseases. But this present study emphasized on adults, they had not very good knowledge regarding infectious diseases. Nurses should engage community adults to equip them in preventing and managing skills of infectious disease.
Nursing practice
Nurses are the backbone of health care set up of any country. The nursing knowledge has gone many evolutions in recent past. The expanded role of professional nurse emphasizes the implication which involves promotive, preventive, curative and rehabilitative aspects. A nurse should involve themselves in regular teaching and counselling session’s foradults and also consider adult people as health care provider for themselves.
Nursing research
A very few interventional studies have been conducted regarding infectious disease.
Knowledge and practice study can be conducted on infectious disease their prevention and management. Comparative study can be conducted in community for infectious disease their prevention and management. New evidenced based information becomes available every level on this subject. It is vital that student research update the knowledge constantly and is always willing to examine and alter their practice in the light of new published evidences.
Nursing administration
Nursing administration may use the study findings to improve the quality of knowledge. The concept of extended role of nurse offer many opportunities for a nurse administrator to improve the knowledge regarding infectious disease their prevention and management among adults in rural community, Gurugram.
DISCUSSION
Health problem do exist with a variety of reasons. The inadequate practices, lack of knowledge about infectious diseases and their prevention, poor socio-economic conditions and poor nutrition are source of factors. In the present study the investigators intended to determine the level of knowledge about infectious diseases and their prevention and management among adults at rural community Gurugram and seek its associations with selected variables. The aim of the study was to assess the knowledge regarding selected infectious disease their prevention and management among adults. Results were consistent with the study conducted by J Ojulong, KH Mitonga and SN Iipinge to evaluate the Knowledge and attitudes of infection prevention and control among health sciences students at University of Namibia. One hundred sixty-two students participated in this study of which 31 were medical, 17 were radiography and 114 were nursing students. Medical students had better overall scores (73%) compared to nursing students (66%) and radiology students (61%). There was no significant difference in scores between sexes or location of the high school being either in rural or urban setting [7].
Results were consistent with other studies which conducted a cross-sectional descriptive survey to assess the knowledge regarding infectious disease management in community Punjab. This study was conducted at 30 adults in the community. Study sample were 30 adults who were recruited through convenience sampling technique who had fulfil inclusion and exclusion criteria. Ethical clearance was taken from the research and ethical committee of the SGL nursing college, Jalandhar. Result of study has shown that knowledge level regarding management of infectious diseases. They had 39 (35.5%) average knowledge, 32(29.1%) had below average, 30(27.3%) had well and very few of them had 9(8.2%) excellent knowledge. This study showed that attitude of adults regarding management of infectious diseases on various level of five point of Likert scale. Study found that highly significant association between level of knowledge and socio-demographic variables i.e. age, qualification, teaching experience, marital status, areas of residence, religion and source of information p-value
CONCLUSION
As the prevention of dengue fever lacks proper vaccine, the main preventive strategy is the awareness building in the community regarding the source reduction process by emptying the man-made containers or dispose those in a systematic or in a proper way. Much efforts to be taken to promote the participation of the community in the action program for eliminating vector-breeding sites as the prevention of dengue fever lacks proper vaccine, the main preventive strategy is the awareness building in the community regarding the source reduction process by emptying the man-made containers or dispose those in a systematic or in a proper way. Much efforts to be taken to promote the participation of the community in the action program for eliminating vector-breeding sitesThe present study attempted to assess the knowledge regarding selected infectious disease their prevention and management among adults in selected Rural Community, Gurugram, Haryana. Out of total study participants 23% of the participants of the total samples were in the age group between 18-22 years of age, 24% of the participants were in the age group between 23-27 years of age. 26% of the participants were in the age group between 28-32 years of age and 27% of participants were in the age group between 33 and above. 62% of the participants were male and 38% participants were female.10% of the participants were illiterate, 46% of the participants were having graduate education, 24% of the participants were having high undergraduate and 20% of the participants were metric.10% of the participants were having self-business, 20% of the participants were homemaker, 46% of the participants were private employee and 24% of the participants were government employee. Source of information through TV 27%, radio 23%, newspaper 31% and friends/others 19 have some knowledge about the infectious disease.
-
Lamballerie DL, Colson P (2006) The battle against infectious diseases in developing countries: The inseparable twins of diagnosis and therapy. Clin Chem 52: 1258-1266.
-
Rashid J, Taiwo OO, Ahluwalia I, Chungong S (2004) Disparities in infectious diseases among women in developing countries. Emerg Infect Dis 10: e24.
-
Shuaib F, Todd D, Stennett DC, Ehiri J, Jolly PE (2010) Knowledge, attitudes and practices regarding dengue infection in Westmoreland, Jamaica. West Indian Med J 59: 139-146. Tulchinsky TH (2014) Communicable diseases. The New Public Health 149-236.
-
Tulchinsky TH (2014) Communicable diseases. The New Public Health 149-236.
-
Centers for Disease Control and Prevention (2011) Ten great public health achievements-United States, 2001-2010. MMWR Morb Mortal Wkly Rep 60: 619-623.
-
Health in India (2010) Causes of death by communicable diseases in India.
-
Ojulong J, Mitonga KH, Iipinge SN (2013) Knowledge and attitudes of infection prevention and control among health sciences students at University of Namibia. Afr Health Sci 13: 1071-1078.
-
Francisco Javier Candel (2018) Teodor EmilovIrene Diaz de la Torre. Update in infectious diseases 2018.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5













QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)


